
![Cost of Medical Billing Services in the USA [2026] Blog Banner](https://curear.com/wp-content/uploads/2025/11/Cost-of-Medical-Billing-Services-in-the-USA-2026-Blog-Banner.webp)
Did you know that the Centers for Medicare & Medicaid Services (CMS) has finalized updates for 2026 requiring U.S. practices to provide clear healthcare cost information and implement transparent billing practices?
The revised CMS transparency regulations are expected to raise the total annual costs of outsourced medical billing services in the U.S. in 2026 to roughly $2,400–$6,000 per provider. This price tag may climb even further as continued healthcare inflation, higher wage costs, and tech and compliance demands drive up overall operating expenses.
It is important to note that the above anticipated costs vary by pricing model and practice factors. This makes it crucial to understand the key billing cost structures, underlying factors, price-setting mechanisms, cost comparisons, and future market trends that will dictate the outsourced billing costs in the U.S in 2026.
This post explains the important nitty-gritties that will impact medical billing pricing in 2026.
Core Cost Structures
Every practice chooses a pricing model that fits its size, specialty, and patient influx. These choices determine whether you pay by percentage, per claim, by subscription, or a full-service fee. Here’s a comparison of the different cost structures at a glance, along with reasonable assumptions:
Assumptions:
- Solo practice’s collections = $250,000–$400,000 / year;
- 3-provider small group collections = $750,000–$1,200,000 / year;
- 10-provider mid-size clinic collections = $2,500,000–$4,000,000 / year.
Claim volumes used for per-claim annualization:
- Solo = 3,000 claims/year,
- 3-provider = 9,000 claims/year,
- 10-provider = 30,000 claims/year.
Billing service provider unit assumptions:
- Percentage fees 4%–8%,
- Flat fee per-claim $3–$8,
- Per-provider subscription $200–$500 / month.
- Onboarding $300–$1,500 per provider (or practice cap $1,400–$1,900).
Cost Structure | Calculation (formula) | Solo (1 provider) Annual $ | 3-provider Annual $ | 10-provider Annual $ |
| Percentage-based (billing service provider takes % of collections) | Collections × 4%–8% | 4% of $250k – 8% of $400k) = $10,000 – $32,000 | 4% of $750k – 8% of $1.2M = $30,000 – $96,000 | 4% of $2.5M – 8% of $4M = $100,000 – $320,000 |
Flat fee per claim | Claims/yr × $3–$8 per claim | 3,000 × $3 – 3,000 × $8 = $9,000 – $24,000 | 9,000 × $3 – 9,000 × $8 = $27,000 – $72,000 | 30,000 × $3 – 30,000 × $8 = $90,000 – $240,000 |
| Monthly subscription/hybrid (per-provider) | Per-provider: $200–$500 / month × no. of providers × 12 | 1 × $200 x 12 – 1 x $500 × 12 = $2,400 – $6,000 | 3 × $200 x 12 – 3 x $500 × 12 = $7,200 – $18,000 | 10 × $200 x 12 – 10 x $500 × 12 = $24,000 – $60,000 |
| Full-service fixed fee (end-to-end RCM) | Billing service provider quote (flat annual) | $5,000 – $20,000 | $15,000 – $60,000 | $50,000 – $200,000 |
Onboarding/setup (one-time) | Per provider or per practice cap | $300 – $1,500 / provider Or $1,400 – $1,900 / practice (cap) | same | same |
Percentage-Based Pricing
Most full-service billing companies charge a percentage of the revenue your practice collects. This provides greater incentives, as billing service providers are paid when your practice is, but the dollar impact grows with higher reimbursements and patient mixes that yield larger claims.
The percentage pricing option is attractive for practices with steady volumes because it shifts risk to the billing company. However, it can be more expensive for rapidly growing or high-reimbursement practices.
Flat Fee Per Claim
Per-claim pricing charges a fixed dollar for each claim submitted. Common ranges range from low single dollars to $8–$10 per claim for complex works. The per-claim fee structure is predictable for high-volume clinics with simple claims. However, it can underpay billing firms for time-intensive appeals and complex coding, which are then billed as add-on fees.
Monthly Subscription or Hybrid Contracts
Subscription (or base + percent) plans bundle services for a steady monthly cost. Small practices often prefer a per-provider monthly fee, while mid-sized groups may accept a hybrid that mixes a low percentage of collections with a flat monthly platform fee. These plans often include reporting and basic denial follow-up, but may charge extra for advanced services.
Full-Service Billing Contracts
End-to-end RCM contracts cover everything from credentialing to patient statements for a single flat monthly or annual fee. These are easiest to budget for but tend to be best suited for larger groups that can justify the fixed cost. Small practices should check for volume minimums and whether appeals and authorizations are fully included.
Factors That Shape Billing Costs
Small changes in who your patients are and how you treat them can move billing costs more than you expect. The following are the core drivers that billing service providers price against:
Claim Complexity
Complex cases take more time to code, verify, and defend, so they cost more to bill. Surgeries, bundled procedures, high-cost drugs, and multi-code encounters require senior coders and extra quality checks, which billing service providers charge for. If your patient panel has higher acuity or multiple chronic conditions, expect more complex claims and higher billing effort.
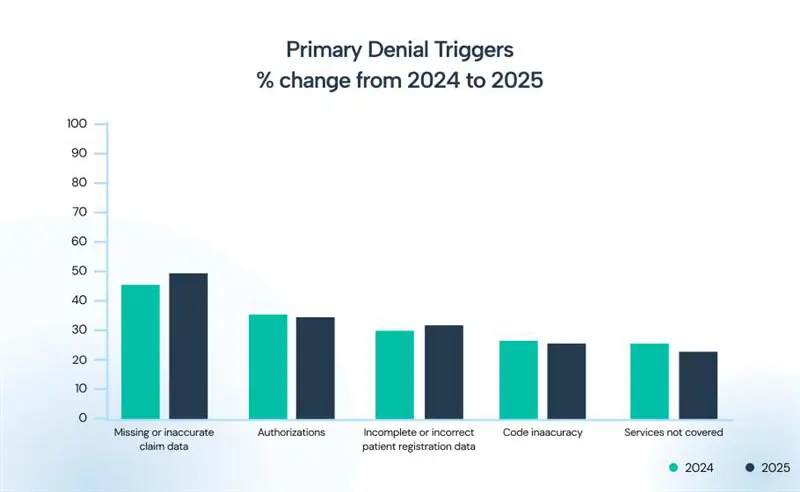
Multiple denial triggers further complicate claim management. For both 2024 and 2025, the list of primary denial triggers remains the same. However, the percentages of their contributions to claim denials have changed, and some have worsened, particularly those related to incorrect and missing data in claims and patient registration.
Denial Management Requirements
Every denied claim usually needs manual research, follow-up, and resubmission, and that work adds up quickly. Practices with frequent prior authorizations, incomplete eligibility checks, or an insurance mix that includes many Medicaid/Medicare patients often see higher denial rates and, therefore, higher billing fees.
Technology Integration Levels
Your EHR, scheduling, and payment systems’ connection to the billing provider affects both onboarding time and ongoing efficiency. Smooth integrations reduce manual data entry and errors, which lowers billing firms’ labor time and your fees. Poor integrations create recurring work that RCM service providers price into their quotes.
Volume Trends
Volume drives per-claim economics. Higher claim volumes usually lower the cost per claim because fixed work is spread more widely. Sudden volume spikes, such as new providers, service lines, or seasonal surges, can temporarily increase costs while medical billing services scale capacity.
Hidden & Overlooked Billing Costs Practices Face
Hidden or overlooked billing costs often hide in routine tasks, turning a reasonable headline fee into a much larger annual expense. Factors like frequent prior authorizations, high denial rates, and demands for custom EHR integration add time and add-on charges that RCM service providers may bill separately.
Authorization Management
Prior authorizations quietly consume staff hours because they entail verifying benefits, submitting requests, tracking approvals, and chasing denials when authorizations lapse. Many billing companies exclude heavy authorization work from base fees or charge per-authorization, so practices with frequent prior authorizations need to pay more than their headline billing rate suggests.
Denial Recovery Work
Denied claims require manual research, payer negotiation, and appeals. Each denial eats staff hours and delays cash. Some billing firms include only first-pass scrubbing in their price and charge extra for appeals or extended follow-up. If your historical denial rate is high, expect added costs, either through higher contract rates or ad hoc recovery fees.
RCM Software Add-Ons
Basic claim submission is often bundled, but advanced features, such as patient payment portals, texting and payment reminders, advanced denial analytics, auto-eligibility checks, or custom EHR connectors, are often extra.
The license or per-user fees can add several hundred to several thousand dollars a year, especially when a practice wants richer reporting or patient-financial engagement tools. Pricing plans of modern RCM software explicitly mention the available add-ons, such as:
1: Clearinghouse Fees
2: eRx Module
3: Patient-pay Portal
4: Advanced BI Package
5: Lab Integration
6: Telehealth Connected
Compliance and Audit Preparation
Staying audit-ready and HIPAA-secure is an ongoing expense that covers regular staff training, periodic chart reviews, documentation corrections, and occasional consultant support. Billing companies may offer “audit support” in name only. Deep remediation or retrospective documentation fixes typically incur extra charges. Budget for periodic compliance work so a single audit doesn’t become a large, unexpected line item.
How Billing Companies Set Prices
Billing service providers don’t guess at the pricing they offer. They build it from data. They look at who your patients are, how you bill, and how much follow-up work your claims usually require. Patient demographics are a core input because they predict claim complexity, denial risk, and likely collections, all of which directly affect the service provider’s labor and technology needs.
Workload Analysis
Billing companies start by estimating the actual work required: charge entry, coding, claim scrubbing, follow-up, and patient billing. They typically ask for a recent sample of claims of 30–90 days to measure time per claim and identify complex cases. The result is an hours-per-claim or tasks-per-claim metric that becomes the foundation of the quote.
Collection Potential Evaluation
Next, billing firms estimate how much cash the practice will realistically collect. That means analyzing payer mix (commercial, Medicare, Medicaid, and self-pay), average reimbursement per claim, and historical payment rates. A practice with low expected collections or many self-pay balances will often receive a different pricing approach than one with high-dollar commercial claims.
Here’s a hypothetical example of how a billing service provider predicts the cash a practice will collect:
| Input | Sample Collection Value (example) | Effect on annual billing cost |
Collections | $350,000 / year | If the billing firm charges % of collections: 6% → $21,000 / year (Range at 4–8% → $14,000–$28,000.) |
Avg claims / year | 3,500 claims/year | If the billing company charges per-claim: $3–$8/claim → $10,500–$28,000 / year At $4/claim → $14,000 / year |
Denial rate | 8% (≈ 280 denied claims) | Extra denial-handling cost: Estimate $20–$50 per denied claim → $5,600–$14,000 At $25/denial → $7,000 / year (May be included or billed extra) |
EHR integration (custom) | Custom API / mapping required | One-time setup $3,000–$10,000 Amortized over 1–3 years = +$1,000–$10,000 in year 1 Amortized over 3 yrs on $6,000 → +$2,000 / year |
The above calculations show why a fixed billing fee can be misleading. Denial work and integration are common add-ons that materially change the final annual cost. If a billing company quotes a percent-of-collections fee, practices must ask whether it includes denial appeals and prior-authorization work. If not, add the denial-handling estimate shown above to your budgeting.
For custom EHR work, practices should ask billing firms to state the one-time setup fee and show the amortized annual impact, making year-1 vs. ongoing costs transparent.
Historical Denial Patterns
Past denial rates and the reasons for denials inform billing service providers of the number of appeals they’ll face. High denial volumes or frequent complex denials lead to more appeals and increased staff time. Hence, RCM service providers incorporate that risk into their prices, sometimes as a higher percentage, and at other times as add-on hourly fees for appeals.
Software and Integration Requirements
Technical work matters. If your EHR, scheduling, or payment system needs custom interfaces, data mapping, or frequent manual exports, billing services include onboarding and maintenance costs. Advanced analytics, automated scrubbing, or a branded patient-payment portal also raise the fee. Simple, well-integrated setups reduce labor and price. Bespoke integrations raise both one-time and recurring costs.
Cost Comparison Between In-House and Outsourced Billing
Choosing between in-house and outsourced billing comes down to control vs. predictability, and your patient demographics (age, payer mix, acuity) also shift the math.
In-House Billing Costs
Hiring billing staff is the biggest recurring expense. A competent medical biller/coder typically costs $45k–$65k/year in salary, plus roughly 25–35% in payroll taxes and benefits. Therefore, a single full-time biller can carry a total payroll burden of $60k–$90k. Add a manager or backup staff, and those numbers grow quickly.
Maintaining coding competency and compliance isn’t free. Certification courses, recertification, and ongoing training (CPC/CPB refreshers, HIPAA, new CPT/ICD updates) typically run hundreds of dollars per person per year, plus paid time for study and workshops.
Software and infrastructure are real line items. Commercial billing modules or dedicated RCM platforms commonly cost hundreds per user per month, clearinghouse connections have per-claim or monthly fees, and desktop/workstation hardware, secure backups, and IT support add both one-time and recurring costs.
Denials and appeals hit home when handled internally. Time spent resolving denials pulls clinical staff or billers away from other work. Studies and billing company reports commonly show that in-house costs per claim are higher than outsourcing costs due to inefficiencies and higher error rates.
Finally, turnover and management overhead matter. Billing teams have above-average churn. Hiring, onboarding, and the lost productivity during transitions are recurring hidden costs you’ll feel in accounts receivable and staff time.
Here’s a summarized version of the estimated in-house billing costs:
| Cost component | Typical annual cost (range) | Notes |
| Billing staff salary + benefits (1 FTE) | $60,000 – $90,000 | Salary $45k–$65k + ~25–35% for taxes/benefits. |
| Coding certifications & training | $300 – $2,000 | Recertification, workshops, and paid study time. |
| Billing software / EHR billing module | $3,600 – $12,000 | Typical $300–$1,000 per user/month, depending on features. |
| Clearinghouse & transaction fees | $300 – $2,000 | Per-claim or monthly connector fees. |
| Workstations, IT & cybersecurity | $1,000 – $8,000 | PCs, VPNs, backups, IT support |
| Denial handling (internal labor) | $3,000 – $15,000 | Depends on the denial rate and the time staff spend on appeals. |
| Compliance, audits & insurance | $500 – $6,000 | Training, external audit prep, cyber/professional insurance. |
| Turnover/hiring costs (annualized) | $2,000 – $10,000 | Recruiting, onboarding, and lost productivity. |
| Estimated total: Solo practice (typical) | $75,000 – $140,000 / year | Sum of the above. Scale up for extra staff or managers. |
Outsourced Billing Costs
Outsourcing converts many of the line items above into a single, predictable fee (a percentage, per-claim, or per-provider subscription). That makes budgeting easier, as practices stop tracking payroll, benefits, workstation costs, and most software licensing for billing purposes.
Practices also outsource hiring, training, and quality control to the billing service providers. Good RCM companies invest in certified coders and denial-management teams, which is why their fee often looks high but can deliver better net collections and fewer write-offs.
Outsourcing often includes software, reporting, access to clearinghouses, and basic integrations as part of the package. That removes IT overhead from your balance sheet, but you should confirm whether advanced analytics, prior-auth handling, or heavy appeals are included or billed extra.
Many billing firms advertise one headline model but bill separately for onboarding, custom EHR mapping, prior-auth work, and extended appeal campaigns. Practices should ask for a sample first-year invoice to understand the true ongoing cost.
Here’s a summarized version of the estimated costs for outsourced medical billing services:
| Cost component | Typical annual cost (range) | Notes |
| Billing service fee percentage model (solo) | $10,000 – $30,000 | Typical market band ~4–8% of collections (use practice $ to convert). |
| Billing service fee per-claim model | $9,000 – $24,000 | $3–$8 per claim → annual depends on claims/yr. |
| Billing service fee subscription/hybrid | $2,400 – $6,000 | $200–$500 per provider/month (solo annualized). |
| Full-service fixed fee (end-to-end) | $5,000 – $20,000 | All-in RCM packages for small practices. |
| Onboarding/setup (one-time, amortized) | $1,000 – $6,000 (Year-1) | $300–$1,500/provider or $1,400–$1,900 practice cap amortized. |
| Denial-handling add-ons (if billed separately) | $5,000 – $14,000 | Often $20–$50 per denied claim. It may be included sometimes. |
| Custom EHR integration (one-time, amortized) | $1,000 – $6,000 (Year-1) | One-time $3k–$10k amortized over 1–3 years. |
| Estimated total: Solo practice (typical) | $12,000 – $35,000 / year | Depends on the chosen model and whether denials/integration are included. |
In-House vs Outsourced Billing: Which is Cheaper?
There’s no universal answer to the above question, but the rule of thumb is that scale and complexity determine the winner. Smaller practices with modest collections and straightforward patient demographics often save money by outsourcing, as they avoid the full salary + software stack. Larger practices or those with highly specialized workflows can sometimes justify an in-house team if they can maintain high utilization and control quality.
Operationally, many groups find the tipping point when they can compare:
- The total fully-loaded cost of in-house billing (salaries + benefits + software + IT + audit risk) versus
- The all-in annual fee of medical billing services (headline fee + known add-ons).
If your internal cost per claim is above the billing service’s quoted per-claim or percent model, or if you cannot maintain staff coverage for denials and compliance, outsourcing usually improves net collections and reduces risk.
For a quick check, run a 12-month comparison using your actual collections, claims/year, denial rate, and a few quotes to show the true dollar impact for your practice.
Market Trends Influencing Billing Costs
Looking ahead to 2026, several industry trends are poised to impact billing costs:
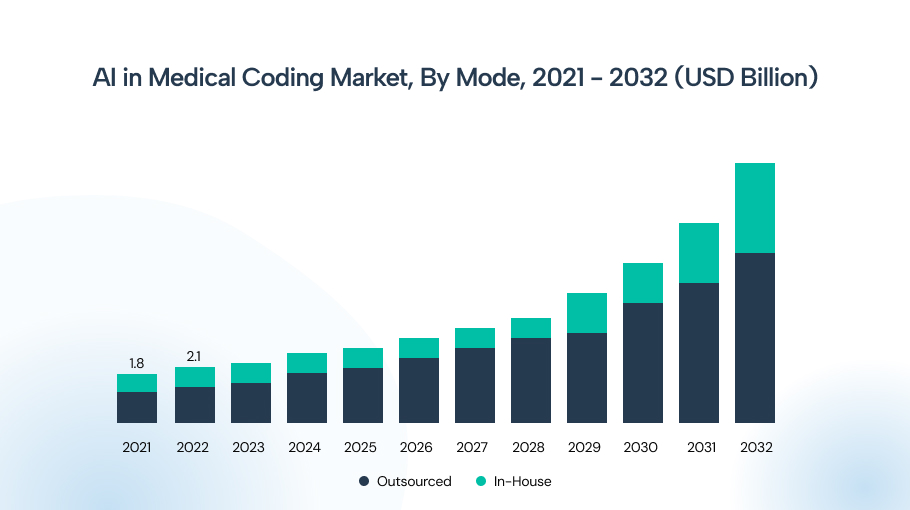
AI Integration
The AI market for medical coding was valued at $2.4 billion in 2023 and is expected to grow at an annual rate of 13.6% from 2024 to 2032. This growth is mainly due to the increasing need for more accurate medical coding, a shortage of skilled medical coders, and a rapid increase in the volume of coding data.
Moreover, the market for AI-enabled medical coding is divided into outsourced and in-house segments, with outsourcing valued at USD 1.7 billion in 2023 and expected to dominate in-house medical billing till 2032.
AI and automation are being adopted across the revenue cycle to reduce routine work and catch errors before claims go out. Expect medical billing services that use advanced scrubbing, NLP coding helpers, and denial-prediction tools to deliver faster first-pass acceptance and fewer reworks, but to charge a premium for that capability.
- What it does: The use of AI in medical billing tasks auto-populates claim fields, flags coding mismatches, prioritizes risky claims for review, and generates appeal drafts.
- Cost impact: Short-term up-front investment (higher prices or implementation fees), which means medium-term lower manual labor per claim.
Practical takeaway for 2026
Practices that accept slightly higher fees for AI-enabled medical billing software will see better cash flow and fewer denials. Practices that resist automation may face rising labor-driven fees.
Increasing Compliance Requirements
Regulatory pressure means more audits, evolving CPT/ICD rules, new prior-authorization mandates, and tighter privacy/security standards, which keep the compliance burden high for every practice.
- What the trend means: More services requiring preauthorization, heightened payer audits, and larger compliance checklists for documentation.
- Cost impact: More training, audit prep, and potential outside consults or compliance services, which means a recurring expense added to billing budgets.
Practical takeaway for 2026
Outsourcing to billing companies with strong compliance programs can stabilize costs, but confirm which audit remedies or retrospective fixes are included and which are billed separately.
National Shortage of Certified Coders
A constrained labor pool for skilled coders and billers pushes wages higher and increases turnover, and that, in turn, feeds directly into pricing.
- Labor reality: Demand for coders is growing faster than average job growth. Experienced coders command higher pay and benefits.
- Cost impact: In-house payroll costs rise. Billing service providers also raise fees as staffing costs increase.
Practical takeaway for 2026
Expect modest upward pressure on billing service rates tied to wage inflation. Billing firms that invest in automation and coder training can limit price increases.
Value-Based Care Models
The shift toward value-based contracts changes what gets billed and how it’s billed. There is now more emphasis on outcomes, quality reporting, and population health data.
- What changes: More quality data capture, diagnosis complexity, and reporting requirements. Less of the revenue is based purely on discrete fee-for-service claims.
- Cost impact: Billing work shifts from volume-driven claim entry to data aggregation, quality-reporting, and analytics. Billing service providers may add reporting fees or repackage pricing for capitated revenue streams.
Practical takeaway for 2026
Billing fees may not drop, but the services included will change, with analytics and outcome reporting becoming standard add-ons.
The Wrap Up
The cost of medical billing services in 2026 will largely reflect current market trends. The percentage-of-collections models range from 5–8% on average, or flat fees of a few dollars per claim. However, every provider’s situation is unique. Patient demographics and practice size heavily shape the final billing cost.
Moreover, hidden factors, like how much time is spent on authorizations or appeals, also add up. On balance, outsourcing remains cost-effective for many practices compared to building an in-house team. When evaluating medical billing partners’ pricing plans, look beyond the headline rate, clarify what’s included, and how your practice’s specific needs might move that rate.
With healthcare costs rising overall and compliance becoming more stringent, planning your 2026 billing budget now is essential.
Frequently Asked Questions
Not strictly required, but outsourcing can save time and improve revenue for small offices. Even solo practitioners often benefit from increased collections and reduced administrative burden.
Ensure transparency on fees and scope. Look for clear coverage of claim submission, denial follow-up, compliance standards, and data security, with no hidden costs for essential tasks.
Many practices see improved cash flow and reduced overhead within 3–6 months after switching. The exact breakeven point depends on ROI in the first year.
Typically, the billing company will send patient statements on your behalf. Make sure patients know the billing contact. Good billers handle patient inquiries and payment plans.
Software and AI can automate billing tasks, but specialized knowledge is key. Most practices use technology plus expert review. Outsourcing often involves AI tools for maximum efficiency.






